
Treat
You have returned to the top of the page.
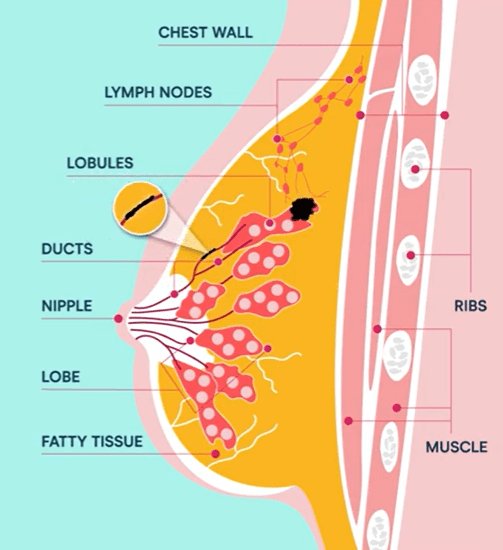
Ductal carcinoma in situ (DCIS) is considered the earliest form of breast cancer. A diagnosis of DCIS means that abnormal cells have been found within the milk ducts of the breast. At this stage, the cells have not broken through the walls of the milk ducts into the surrounding breast tissue. If this happens, the cancer is known as invasive ductal carcinoma (IDC).
Whilst a diagnosis of DCIS can happen to anyone, there are risk factors associated with all breast cancers that may increase the chance of developing DCIS. These are:
As a non-invasive, ‘stage 0’ breast cancer, this cancer itself is not life threatening. However, having DCIS does increase the chance of developing invasive breast cancer later in life, which can be life threatening if left untreated. Generally, the five-year survival rate for ductal carcinoma in situ is 100%.
DCIS generally does not result in any signs or symptoms. It is most commonly discovered through breast screening mammograms or an ultrasound. However, ductal carcinoma in situ can occasionally be found following a change in the breast such as a lump or discharge from the nipple. If these symptoms do occur, it’s more likely that it will be invasive breast cancer. In Australia, research showed that women who have had DCIS are 3.9 times more likely to develop invasive breast cancer than someone who has never had breast cancer.
If you experience any of these symptoms, or further changes in the breast such as an area of puckered, thickened or unusual skin, it is recommended to seek medical attention.
Ductal carcinoma in situ is generally diagnosed via the following methods:
The majority of cases of DCIS are diagnosed with a mammogram. The mammogram detects tiny specks of calcium known as calcifications which come from a build-up of older cancer cells and will appear as dark shadows or white specks.
If the mammogram does appear suspicious your doctor may recommend a biopsy. This involves taking a small sample of cells or tissue from the area of concern in the breast, which is then examined by a pathologist. The pathologist will determine if there is cancer and identify the grade (how abnormal the cells look and how fast they are growing) of the DCIS, and the type, the hormone receptor status.
As with all types of cancer, ductal carcinoma in situ is categorised into stages and grades. The staging system describes how far the cancer has spread beyond its original location. As DCIS is non-invasive, it is always categorised as Stage 0. The grading system categorises the cells based on how much they resemble normal breast cells, and how quickly they are growing.
Grade 1 DCIS cells closely resemble normal cells and tend to grow slowly. Low grade DCIS can sometimes be referred to as ‘non-comedo’ DCIS. ‘Non comedo’ indicates that there are not many dead (necrotic) cancer cells inside the tumour. Other patterns of DCIS are referred to as papillary DCIS (cells arranged in a finger like pattern), cribriform DCIS (empty spaces between the cancer cells in the tissue – a swiss cheese appearance) and solid DCIS (cancer cells completely fill the breast ducts)
Grade 2 DCIS cells look less like normal cells and grow faster than them. Moderate grade DCIS can sometimes be referred to as grade 2 ‘non-comedo’ DCIS. ‘Non comedo’ indicates that there are not many dead (necrotic) cancer cells inside the tumour. Other patterns of DCIS are referred to as papillary DCIS (cells arranged in a finger like pattern), cribriform DCIS (empty spaces between the cancer cells in the tissue similar to swiss cheese) and solid DCIS (cancer cells completely fill the breast ducts)
Grade 3 DCIS cells look very different from normal cells and grow faster than them. High Grade DCIS can sometimes be referred to as ‘comedo’ or ‘comedo necrosis’. which refers to the presence of dead (necrotic) cancer cells that build up inside the tumour.
Whilst a diagnosis of ductal carcinoma in situ is not life threatening, the increased risk of developing invasive breast cancer means that treatment is recommended. The aim of treating DCIS is to prevent invasive breast cancer from developing, as this can spread beyond the milk ducts and to other parts of the body, where treatment becomes much more difficult.
Treatment for ductal carcinoma in situ breast cancer depends on several factors, such as the size of the cancer in relation to the breast, the grade of the DCIS and the woman’s individual circumstances such as age and family history. Some of the treatment options which may be recommended are:
Breast cancer surgery is one of the most common treatments to be recommended for DCIS. One of the following types of surgery may be recommended:
Also known as breast conserving surgery, a lumpectomy involves the removal of the DCIS and an area of healthy breast tissue surrounding the cancer, known as the surgical margin. After the surgery, the surgical margin is examined to determine how likely it is that there are any further cancer cells in the breast. If cancerous cells are detected, more surgery may be recommended.
A mastectomy is a less common treatment for DCIS but may be recommended if the DCIS has spread beyond the milk ducts to the surrounding breast tissue.
After surgery for DCIS, follow up therapies may be recommended to reduce the risk of the cancer returning or progressing to invasive cancer. These may include:
Radiation therapy is often recommended after a lumpectomy. This involves the use of X rays to kill cancer cells.
Hormone therapy may be recommended as an additional treatment given after surgery or radiation, used to reduced the chances of the cancer returning. Hormone treatment slows or blocks the action of estrogen in order to prevent the continued growth of cancer cells and reduce the risk of invasive breast cancer developing. Estrogen can fuel the growth of some breast cancer cells, so hormone therapy can prevent estrogen from reaching the cancer cells or by shutting down the estrogen receptor on breast cancer cells. This treatment is only effective against cancers that grow in response to hormones. Hormone therapy drugs include tamoxifen and aromatase inhibitors.
The chance of DCIS returning dependents on various factors. Factors that can increase the risk of recurrence are:
Ductal carcinoma in situ breast cancer is a form of early breast cancer which is contained within the milk ducts of the breast. This cancer is referred to as non-invasive and is the earliest form of breast cancer.
Ductal carcinoma in situ is not a life threatening diagnosis and has a very high survival rate of 100%. However, having DCIS does increase the risk of developing invasive breast cancer, which can be very serious if not
In most cases, DCIS does not present with any symptoms. However, in a very small number of cases, there may be a lump in the breast or an unusual
There are several known risk factors which may increase the likelihood of developing DCIS, one of which includes a family history of breast cancer.
Most women with ductal carcinoma in situ experience no pain. or notice any other symptoms. However, in some cases there may be an unusual lump or discharge from the nipple, which may be uncomfortable.
Ductal carcinoma in situ is a type of breast cancer. It is also referred to as non-invasive or pre-invasive cancer as the cells have not spread to any other location beyond the milk ducts.
The speed in which ductal carcinoma in situ grows depends on specific features of the cancer cells and can be classified as the grade of the cancer. The grades range from 1 to 3, with 1 meaning slow growing and 3 meaning a rapidly growing cancer.
If DCIS is left untreated, there is a higher risk that it can develop into invasive breast cancer, which can spread to other parts of the body.
The difference between ductal carcinoma in situ and invasive ductal carcinoma is that ductal carcinoma in situ is located within the milk ducts of the breast and has not spread into the surrounding breast tissue. Invasive ductal carcinoma is breast cancer that has spread from the milk ducts to the surrounding breast tissue of further.